2025: Volume 5, Issue 1
Current Issue
 Abstract
Abstract  PDF
PDFTraumatic Avulsion of the Anterior Inferior Iliac Spine with Secondary Bony Hypertrophy in a 15-Year-Old Football Player: A Case Report
Mohamed Mokhtar Jmal*, Dera Andraina Ratsimandresy, Hachem Ben Aayech, El Mostafa Laalla
Department of Orthopedic and Trauma Surgery, Centre Hospitalier de Verdun Saint Mihiel, Verdun, France
*Corresponding author: Dr. Mohamed Mokhtar Jmal, Department of Orthopedic and Trauma Surgery, Centre Hospitalier de Verdun Saint Mihiel, 46 Ter Côte Saint Barthélémy, 55100 Verdun, France, Tel: 0626789591, E-mail: [email protected]
Received Date: November 05, 2025
Publication Date: November 18, 2025
Citation: Jmal MM, et al. (2025). Traumatic Avulsion of the Anterior Inferior Iliac Spine with Secondary Bony Hypertrophy in a 15-Year-Old Football Player: A Case Report. Surgeries. 5(1):13.
Copyright: Jmal MM, et al. © (2025).
ABSTRACT
Introduction: Apophyseal avulsion fractures of the pelvis predominantly occur in adolescent athletes due to skeletal immaturity. The anterior inferior iliac spine (AIIS) is a rare but characteristic site of injury. Case Presentation: We report the case of a 15-year-old male football player who sustained a traumatic avulsion of the right AIIS. The diagnosis was confirmed radiologically, and the patient was managed conservatively. Results: The clinical course was favorable, with a return to sports at three months. Conclusion: Early diagnosis and conservative management typically allow full recovery in most cases.
Keywords: Avulsion Fracture, Anterior Inferior Iliac Spine, Adolescent, Football, Orthopedics
INTRODUCTION
Apophyseal avulsion fractures of the pelvis are uncommon, representing approximately 1–5% of pelvic injuries in adolescent athletes [1]. They typically occur during sudden, forceful muscle contractions in sports requiring explosive movements, such as football, sprinting, or gymnastics.
The AIIS serves as the insertion site of the direct head of the rectus femoris muscle. Traumatic avulsion can occur during forceful kicking or resisted shooting [2]. We present a case of traumatic AIIS avulsion in an adolescent football player, along with a review of the literature.
MATERIALS AND METHODS
This is a single-center observational study reporting an isolated clinical case managed in a trauma emergency department. Clinical, radiographic, and follow-up data were retrospectively collected from the patient’s medical record.
CASE PRESENTATION
A 15-year-old right-handed male with no significant medical history presented with sudden right hip pain following a high jump while attempting to head the ball.
Clinical findings included:
- Localized tenderness over the anterior hip region
- Painful limitation of active hip flexion with complete functional impairment
- No neurological or vascular deficits
Standard pelvic radiography revealed a displaced bony fragment at the right AIIS. CT scan confirmed the avulsion fracture without intra-articular involvement or adjacent soft tissue injury.
Management: The patient underwent strict rest, analgesia, icing, and partial weight-bearing with crutches for 30 days. Progressive weight-bearing was initiated at three weeks, followed by functional rehabilitation.
During follow-up, a spontaneous snapping was noted at the AIIS during activity, associated with mild bony hypertrophy at the avulsion site, confirmed on CT and MRI. No persistent pain or joint impingement was observed. The bony hypertrophy represented an adaptive consolidation response and did not impair functional recovery (Figures 1-6).
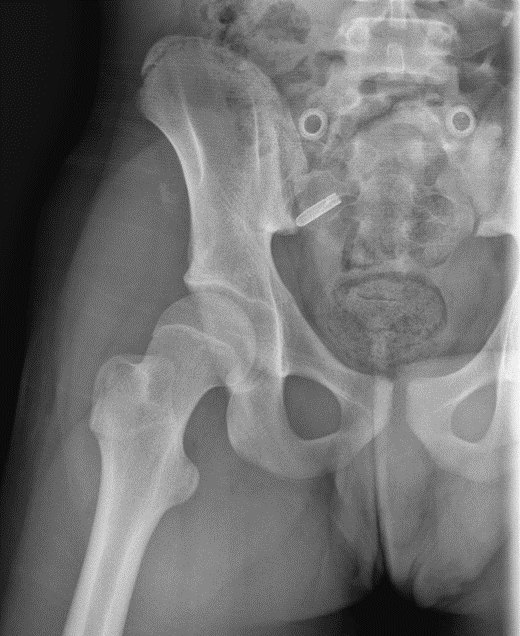
Figure 1. Initial radiograph of the right hip: epiphyseal separation of the anterior inferior iliac spine.
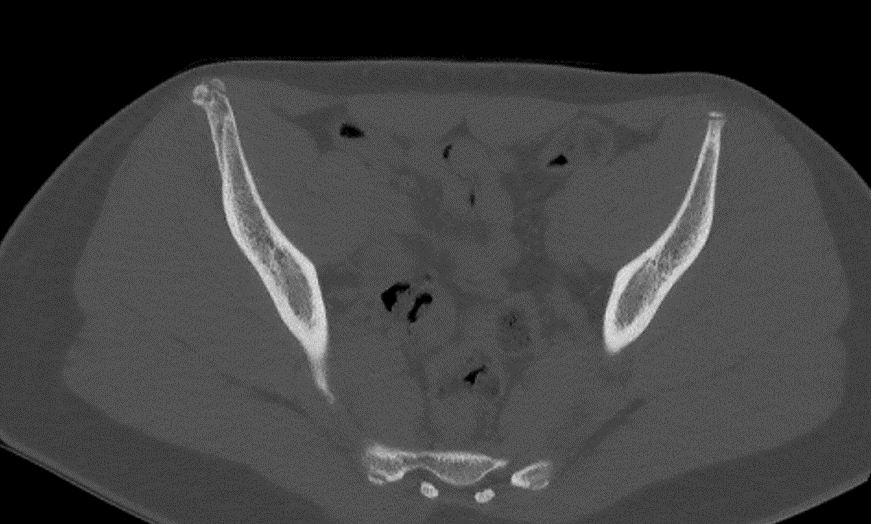
Figure 2. CT scan initial axial slice: EIAI avulsion.

Figure 3. X-ray of the right hip 1 month post-traumatic.

Figure 4. X-ray of the right hip 8 months post-traumatic.
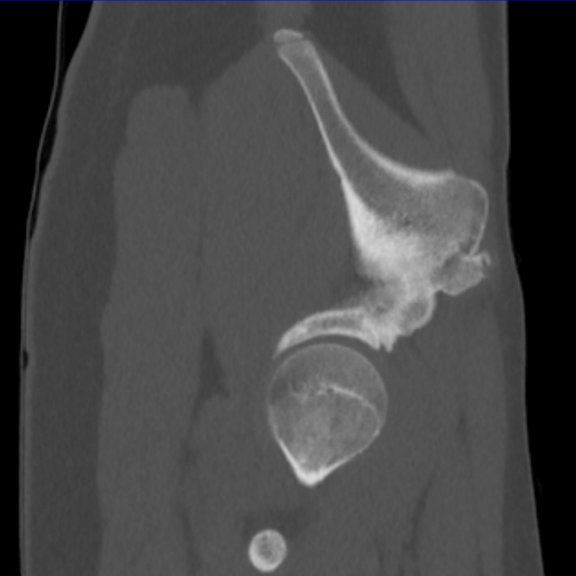
Figure 5. Pelvic CT scan at 6 months post-traumatic.

Figure 6. Pelvic CT scan at 6 months post-traumatic.
DISCUSSION
Apophyseal avulsion fractures occur almost exclusively in adolescents, when the growth plate is biomechanically weaker than the tendon [3]. The AIIS is commonly affected in football players due to eccentric contraction of the rectus femoris during kicking [4].
Diagnosis: Conventional radiography is usually sufficient; MRI may be indicated to clarify fragment displacement or assess associated soft tissue injury.
Management: Conservative treatment is the standard of care. Surgery is rarely required, reserved for significant fragment displacement (>2 cm) or complications such as nonunion, malunion, or secondary femoroacetabular impingement [5].
Prognosis: Most patients return to sports within 8–12 weeks [6]. Post-avulsion bony hypertrophy reflects periosteal and ossification center adaptation and is usually asymptomatic, as in our case [7,8]. Radiographic follow-up is recommended to rule out symptomatic malunion or nonunion.
Our observation confirms that non-operative management leads to complete functional recovery and safe return to sport.
CONCLUSION
AIIS avulsion fractures are rare but characteristic injuries in adolescent athletes, particularly in football. Diagnosis relies on clinical assessment and standard radiography. Conservative management is effective in most cases, with an excellent functional prognosis.
ACKNOWLEDGEMENTS
None.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
- Rossi F, Dragoni S. (2001). Acute avulsion fractures of the pelvis in adolescent competitive athletes: prevalence, location and sports distribution of 203 cases collected. Skeletal Radiol. 30(3):127-131.
- Schuett DJ, Bomar JD, Pennock AT. (2015). Pelvic Apophyseal Avulsion Fractures: A Retrospective Review of 228 Cases. J Pediatr Orthop. 35(6):617-623.
- Kujala UM, Orava S. (1993). Ischial apophysis injuries in athletes. Sports Med. 16(4):290-294.
- Sundar M, Carty H. (1994). Avulsion fractures of the pelvis in children: a report of 32 fractures and their outcome. Skeletal Radiol. 23(2):85-90.
- Serbest S, Tosun HB, Tiftikçi U. (2016). Avulsion fracture of the anterior inferior iliac spine in adolescents: a report of two cases and review of the literature. Case Rep Orthop. 2016:7045362.
- Eberbach H, Hohloch L, Feucht MJ, Konstantinidis L, Südkamp NP, Zwingmann J. (2017). Operative versus conservative treatment of apophyseal avulsion fractures of the pelvis in adolescents: a systematic review with meta-analysis of observational studies. Knee Surg Sports Traumatol Arthrosc. 25(12):3749-3757.
- Clemente A, et al. (2020). Bone hypertrophy after avulsion fractures of the pelvis in adolescents. J Pediatr Orthop. 40(5):e381-e386.
- Kim H, et al. (2019). Post-traumatic osseous overgrowth in adolescent pelvic fractures: clinical implications. Skeletal Radiol. 48(10):1575-1582.